 |
Research Article
Barriers to utilization of skilled birth attendance among post-natal women in a North Horr ward, Marsarbit County, Kenya: A cross-sectional study
1 Department of Health Systems, Amref International University, School of Public Health, Nairobi, Kenya
Address correspondence to:
Kame Wato Kofo
Amref International University, Department of Health Systems, School of Public Health, Nairobi,
Kenya
Message to Corresponding Author
Article ID: 100012M01KK2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Kofo KW, Matiang’i M, Akolo M. Barriers to utilization of skilled birth attendance among post-natal women in a North Horr ward, Marsarbit County, Kenya: A cross-sectional study. Edorium J Matern Child Health 2024;8(2):1–11.ABSTRACT
Aims: The purpose of this study was to examine barriers to the utilization of skilled birth attendance among women in North Horr ward, Marsarbit County. Specific aims were to assess potential demographic, economic, sociocultural, and health facility barriers that facilitate home deliveries.
Methods: A mixed methods approach was used. A survey questionnaire captured quantitative data from 306 women, while 15 semi-structured interviews were conducted to support the quantitative findings. Quantitative data were analyzed through descriptive and inferential statistics using Stata version 15, while qualitative data were analyzed thematically using NVIVO and presented in tabular form.
Results: A total of 306 women participated (mean age=33 years). 92% (n=281) were married, 97% (n=297) had children, unemployment was 98% (n=300). Age, costs of transport, poor infrastructures, lack of money, and all health-related factors were significantly associated with place of delivery (p<0.0001). 50% (n=153) reported health facility as place of last delivery, 47% (n=144) delivered at home, though sociocultural factors like traditional birth attendant (TBA) availability (80% [n=123]) influenced the choice. The regression model showed no significant relationships for sociocultural barriers (p>0.05). Qualitative findings revealed financial constraints, sociocultural norms, and health infrastructure deficits as major barriers to skilled birth attendance utilization.
Conclusion: Multifaceted barriers interact as barriers to the utilization of skilled birth attendance among women in North Horr ward, Marsarbit County. Initiatives aimed at improving skilled birth attendance utilization must judiciously tackle poverty, remoteness, inconsistent quality care and traditional mindsets.
Keywords: Economic barriers Health-facility barriers, Maternal healthcare utilization, Skilled birth attendance, Sociocultural barriers
Introduction
Unskilled birth attendance remains a significant challenge for public health systems globally, impeding efforts to reduce maternal and infant mortality. Unskilled birth attendance is a leading factor in avoidable maternal and infant deaths [1]. Although 85% of births worldwide are assisted by skilled personnel, there are stark regional disparities, with Asia, Northern America, and Europe nearing universal coverage, while sub-Saharan Africa lags with only 64% skilled birth attendance [2]. In 2016, approximately 303,000 women died from pregnancy-related complications, with 99% of these deaths occurring in developing countries [3]. Unskilled birth attendance is a major promoter of maternal morbidity and mortality as recognized by search.
Southern Asia and Africa accounted for 86% of global maternal mortality in 2017, with sub-Saharan Africa alone contributing 66% of these deaths. This was attributed to inadequate care during pregnancy and childbirth [3]. In sub-Saharan Africa, limited access to skilled labor, particularly in rural areas, contributes to over 300,000 pregnancy-related deaths annually [4],[5]. The survival rate for infants also varies significantly by region, with sub-Saharan Africa having the highest infant mortality rate at 27 deaths per 1,000 live births in 2020 [6].
In Kenya, the maternal mortality ratio and infant mortality rate are 362 per 100,000 and 22 per 1,000 live births, respectively. Amid these devastating statistics, only 61.2% of births occur in health facilities in Kenya [7]. Despite government efforts to improve maternal and neonatal health services, there remains a decline in women giving birth in medical facilities, especially in remote parts of the country [8]. In 2013, Kenya had 289,000 maternal deaths [8]. The fifth Millennium Development Goal aimed for a 75% reduction in maternal mortality by 2015, a target Kenya has struggled to meet [9]. Maternal deaths in Kenya are around 488 per 100,000 live births, far from the target of 147 per 100,000 [9].
Despite introducing the free maternity care policy in 2013, which increased facility-based births from 44% in 2008 to 61% in 2014 [8],[9], significant regional disparities persist. The Linda Mama program, which ensured free access to maternity services at public health facilities, significantly helped reduce home deliveries attended by traditional birth attendants (TBAs) [10]. However, challenges such as lack of awareness and enrollment in the National Hospital Insurance Fund (NHIF) scheme hindered access to these services in remote areas [11]. Other challenges especially related to delayed disbursements of health facility reimbursements also caused lapses in continuity of care in many parts of the country.
In Marsabit County, unskilled birth attendance remains prevalent. Despite antenatal care counselling, only 13% of women delivered at health facilities in 2021 and 2022 in North Horr ward [12]. This exposes mothers and newborns to severe risks, including maternal and infant mortality and long-term health issues [13]. Factors contributing to the high rate of unskilled home deliveries include cultural preferences, inadequate health facilities, and logistical challenges [10],[14].
The literature highlights various factors contributing to the persistent use of unskilled birth attendances (UBAs) in Kenya, particularly in rural areas. UBAs, often without formal training, provide essential support during childbirth, especially in regions with limited healthcare access [13],[14]. Sociocultural influences, such as traditional beliefs and the need for spousal permission, significantly impact women’s choices [15]. Economic barriers, including transportation costs and poverty, further exacerbate the reliance on UBAs [16]. Healthcare system deficiencies, such as inadequate service quality and staff shortages, also deter women from seeking skilled birth attendants [14],[17]. Despite policies advocating for UBAs to transition to supportive roles, their use remains prevalent due to the perceived inadequacy of formal healthcare services [18],[19]. Studies show that maternal education influences the likelihood of seeking skilled care, with educated women more likely to use professional services [12],[20]. This situation underscores the need for comprehensive strategies addressing the multifaceted barriers to skilled birth attendance as outlined in the Health Belief Model [21].
This study aimed to investigate the barriers to utilizing skilled birth attendance services among women in North Horr ward, Marsabit County. By understanding the demographic, economic, sociocultural, and health facility-related factors that influence the utilization of maternal healthcare services, the study sought to inform policymakers and stakeholders on effective strategies to improve maternal and child health outcomes. This study thus aligned with national and global health goals by aiming to support the attainment of sustainable development goal.
MATERIALS AND METHODS
Study design
The study employed a cross-sectional design with a mixed-methods approach. Quantitative data were collected using structured questionnaires designed to gather information on skilled birth attendance while qualitative data were obtained through key informant interviews with community health volunteers, traditional birth attendants, and the area leaders. This approach targeted females aged 15–49 years to provide a thorough understanding of reproductive health practices. Triangulation ensured a robust exploration of the factors influencing skilled birth attendance.
Study site
The research was conducted in North Horr, a sub-county in Marsabit County, Kenya. North Horr is the largest sub-county in Marsabit County by geographical size, with a population of 71,447 as of the Kenya Census 2019. The area includes five wards—Illeret, Dukana, North Horr, Maikona, and Turbi—each with distinct health facility distributions. The selection of North Horr was based on its high rates of home deliveries and associated negative outcomes, making it a critical area for studying skilled birth attendance.
Study population
The target population comprised postnatal women aged 15–49 years, with a focus on those who had delivered within the last six months. The estimated target population was approximately 5,000, according to the 2019 census, representing 29% of the total population of North Horr ward. Key informants, including community elders, were also targeted. The sample size of women was determined using Fisher’s formula, resulting in a target of 327 women after adjustments for non-response [22]. For qualitative data, a sample size of 15 key informants was chosen based on the suggestions of other studies. Typically, saturation in qualitative research occurs between 12 and 15 interviews [23]. The women included in the study were selected using cluster random sampling whereas key informants were selected using a purposive sampling approach.
Data collection instruments
Data collection instruments included structured questionnaires for quantitative data and interview guides for qualitative data. The questionnaires were administered via the Kobo-Collect tool. Qualitative data were gathered through structured interviews with key informants.
Data analysis
Data processing involved sorting, coding, and analyzing data using Stata Version 15 for quantitative data and NVIVO for qualitative data. Whereas numerical data were analyzed using descriptive and inferential statistics, qualitative data were analyzed thematically.
Ethical considerations
Ethical approval was obtained from relevant authorities, including the Amref Health Africa Ethics and Scientific Review Committee (ESRC P1442/2023). Informed consent was sought from all participants while measures were implemented to ensure voluntary participation, privacy, and confidentiality.
RESULTS
Influence of participant demographics on the utilization of skilled birth attendance
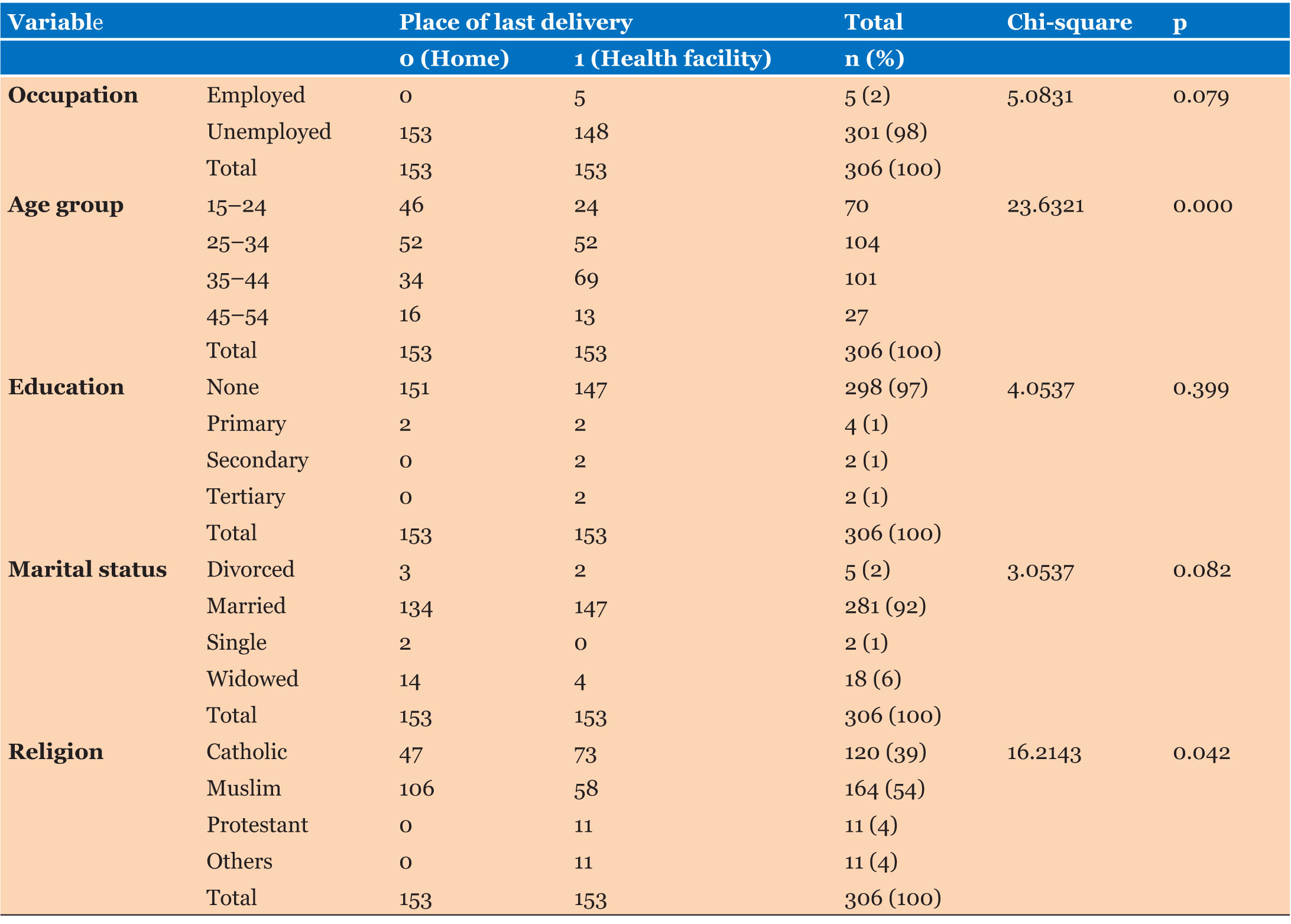
The age data represent values for 306 individuals. The mean age is 33 years old, with a standard deviation of 8.7 years. This indicates there is a fair amount of variation in ages, but most individuals are centered around 33 years old. The minimum age was 19 and the maximum was 49. Looking at marital status, the majority of individuals are married (92% [n=281]), 6% (n=18) were widowed, 2% (n=5) were divorced, and only 1% (n=2) were single. As for children per family, 97% (n=297) reported having children, while only 3% (n=9) had no children. For those with children, the mean number of children was 3.5, indicating that families tended to be large. Most participants were unemployed (98% [n=301]) while the majority were Muslims (54% [n=164]). It was also striking that a whopping 97% (n=298) had no education at all. The chi-square test of independence provided an analysis of the association between the “Place of Last Delivery” and the demographic variables. Age group and religion were noted to be associated with the place of last delivery (p<0.05) (Table 1).
Economic factors affecting utilization of skilled birth attendance
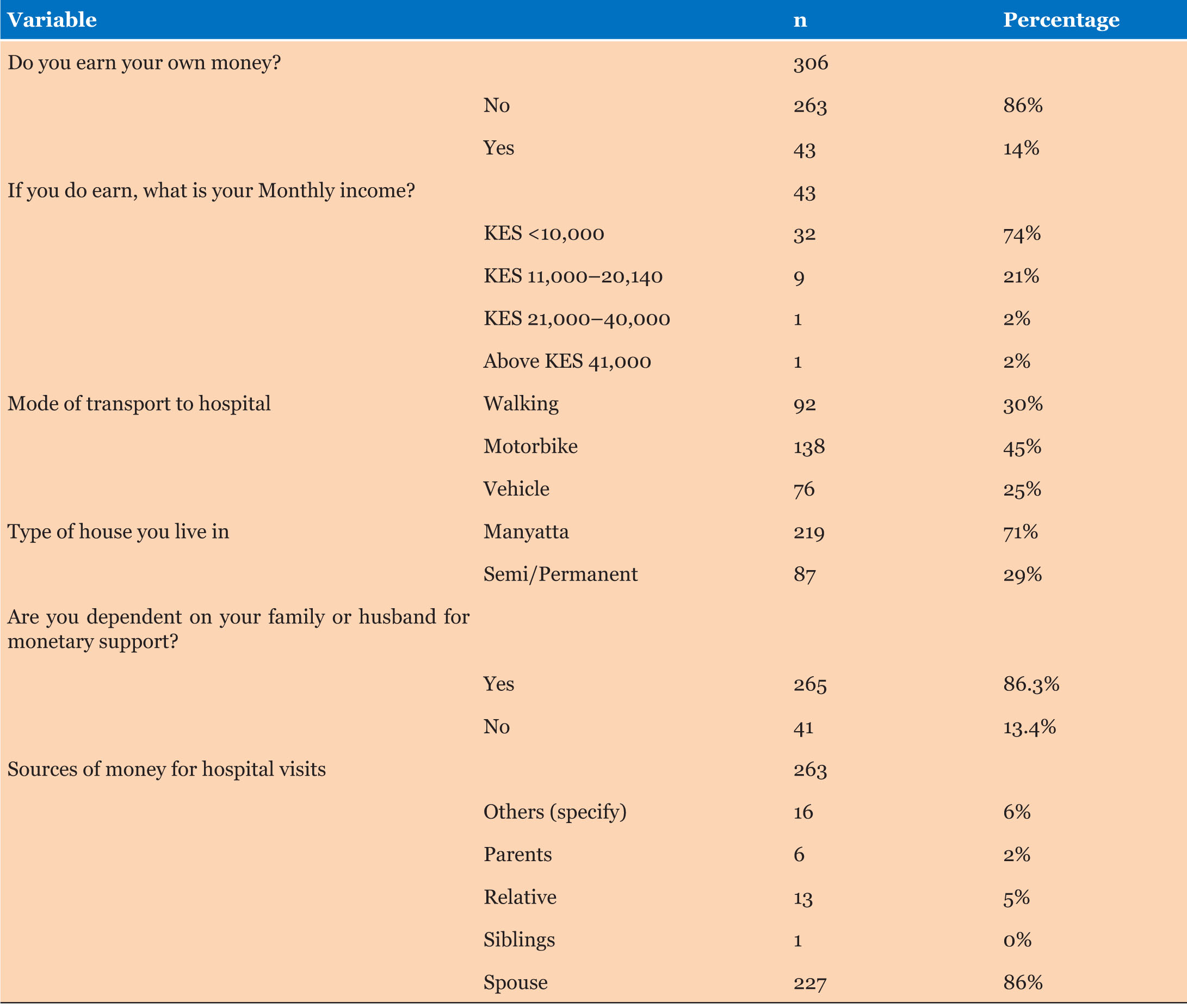
The data revealed significant economic constraints affecting women’s access to skilled birth attendance. A substantial majority (86% [n=263]) of women did not earn their income, relying heavily on their husbands (87% [n=263]) or other family members. Of the 14% (n=43) who did earn money, 74% (n=32) made less than KES 10,000 monthly, highlighting widespread low income. Transportation posed a significant barrier, with most women (71% [n=219]) living in manyattas and relying on walking (30% [n=92]) or motorbikes (45% [n=138]). Insufficient funds (77% [n=236]), high transport costs (38% [n=117]), and poor transportation (34% [n=104]) were the primary obstacles to healthcare access reported by women. The chi-square test showed significant associations between these economic factors and delivery locations, underscoring the impact of financial hardship on healthcare choices (p<0.05) (Table 2). Qualitative data supported these findings, with participants citing prohibitive formal and informal costs as barriers. For instance, P7 lamented, “Many people are unemployed and unable to go to good hospitals due to lack of resources.” Similarly, P14 noted, “I had to sacrifice income from not working for several days to stay at the hospital after delivery, which was a financial burden.”
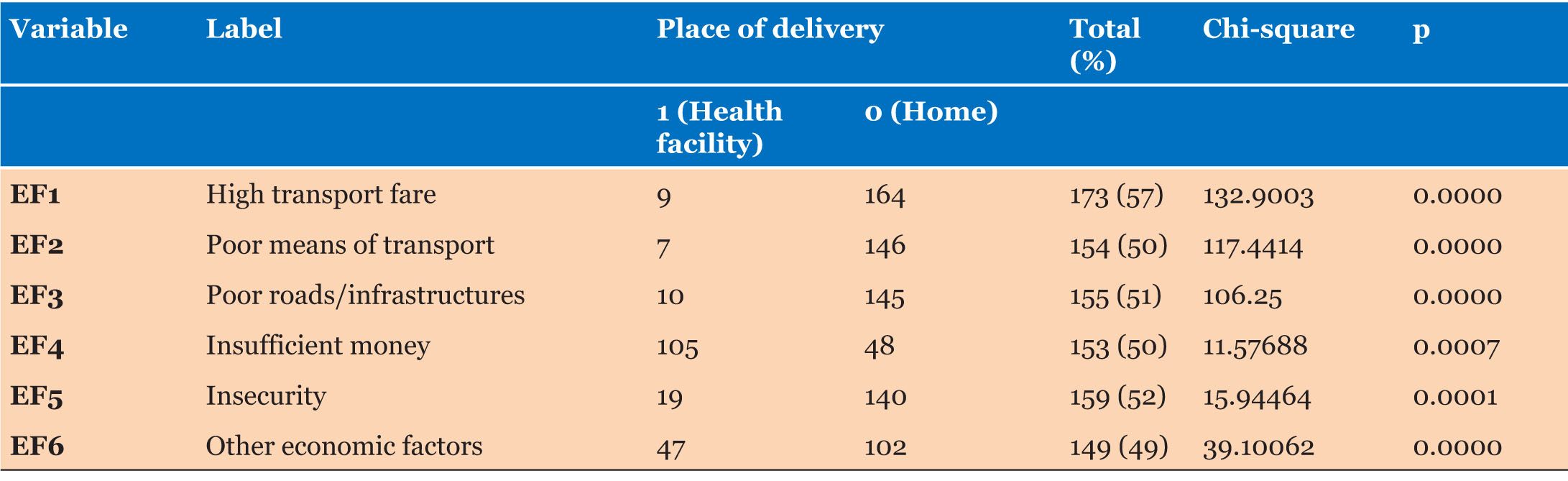
The chi-square analysis of economic barriers revealed significant associations with delivery locations. High transport costs were cited by 57% (n=173/306) of women, while poor means of transport were reported by 50% (n=154/306) of women. Poor roads and infrastructures were noted by 51% (n=155/306) of women and a further 50% (n=153/306) of women cited insufficient money to pay for transport and services as a significant issue. Other economic-related barriers included insecurity reported by 52% (n=159/306), and other unspecified economic factors reported by 49% (n=149/306) of women. All these economic factors were significantly associated with the place of last delivery (p<0.0001). These findings underscore the profound impact of economic barriers on women’s access to skilled birth attendance (Table 3).
Sociocultural factors that affect the utilization of skilled birth attendance
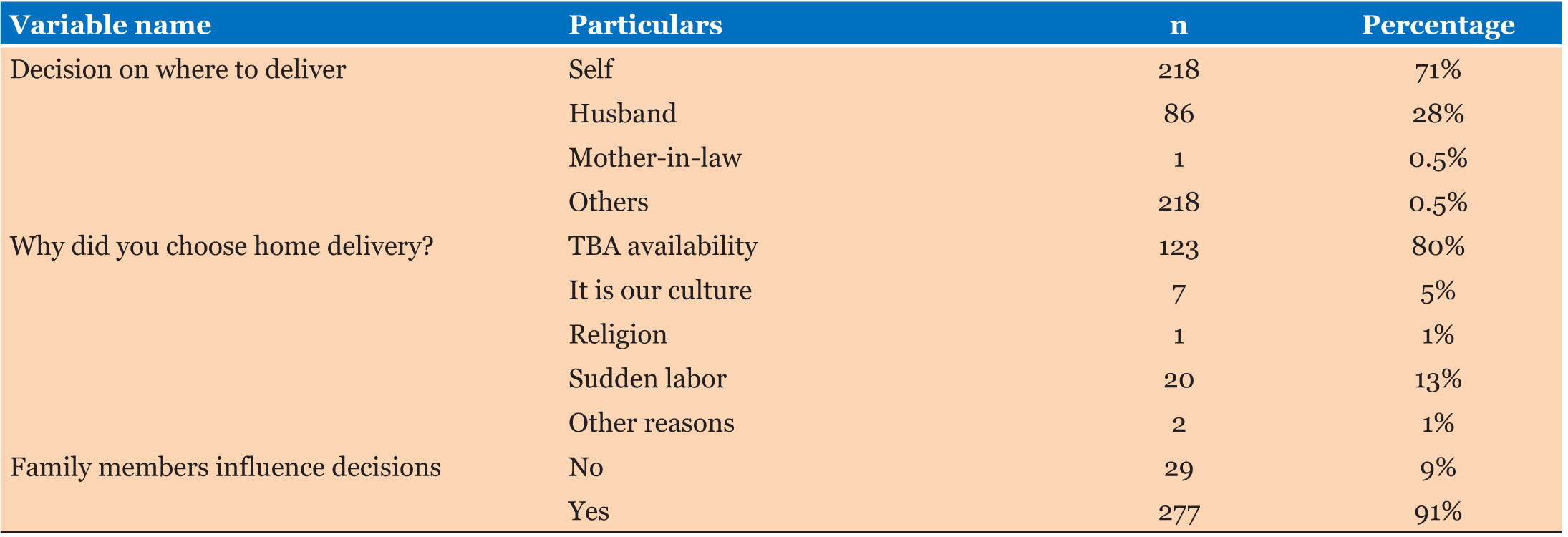
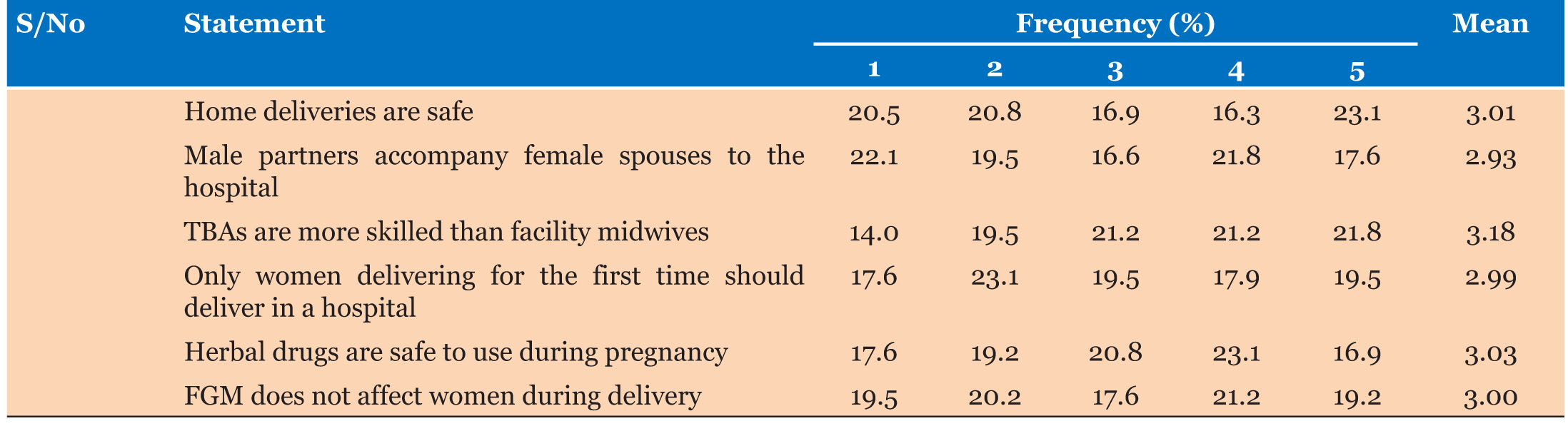
A key decision factor for place of delivery was who determines where the woman gives birth. Although most women (71% [n=218]) reported they made the decision themselves, 28% (n=85) said their husbands decided. This indicated that male partners play a sizable role in the choice to deliver at a facility or home. For those opting for home delivery, the most common reason was the availability of traditional birth attendants (TBAs) where health facilities were far away (80% [n=123]). Still, tradition appeared to be leading many women, especially in rural areas, to depend on TBAs over formal medical care. The data also highlighted the influence family can have over maternal decisions and behaviors. Most women (91% [n=277]) reported getting advice from family members, showing they value input on delivery options (Table 4). A Likert scale question was also used to assess women’s cultural aspects and perspectives that influenced their choices to use skilled or unskilled birth attendants (Table 5).
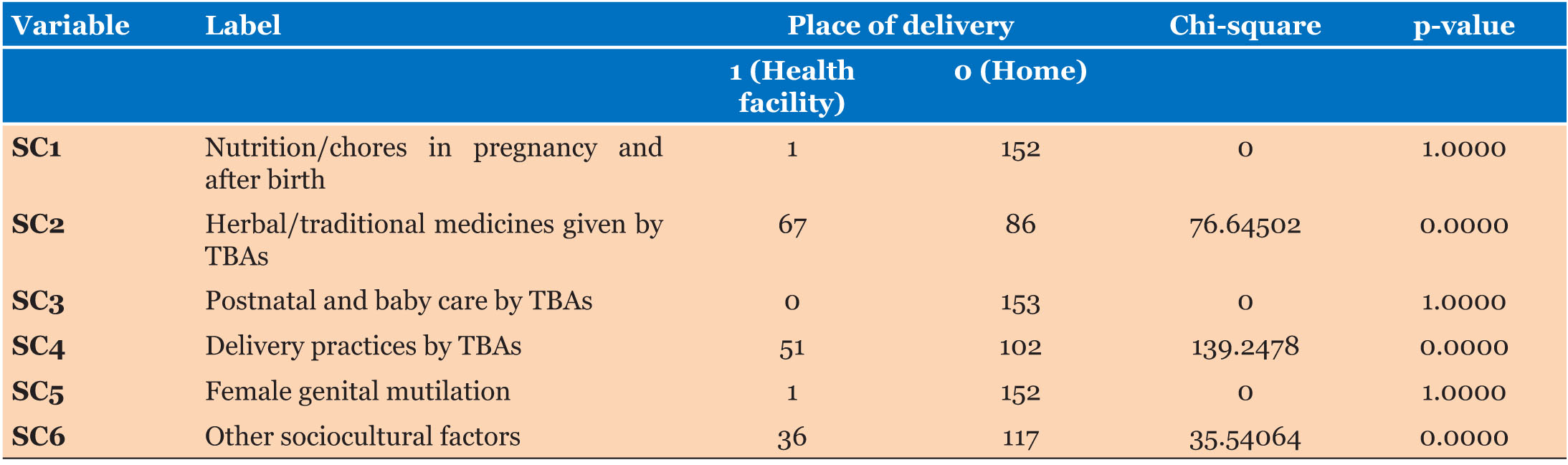
There was a significant association between sociocultural factors and delivery locations (Table 6). Notably, delivery practices by TBAs and the use of herbal/traditional medicines given by TBAs exhibited a statistically significant relationship with the place of last delivery (p<0.001). Conversely, nutrition/chores in pregnancy and after birth done by TBAs, postnatal and baby care, female genital mutilation (FGM), and other sociocultural factors did not show a significant relationship with the place of delivery although they were also significantly reported. These findings emphasize the nuanced influence of sociocultural factors on healthcare choices in the community.
The qualitative analysis also unearthed deeply entrenched sociocultural barriers hindering the uptake of skilled birth attendance. A poignant perspective emerged from a community health volunteer (CHV), encapsulating the prevailing cultural aversion toward hospital deliveries: “Cultural practice dislikes hospital deliveries.” This sentiment underscores the preference for home births facilitated by TBAs in the community. The community generally considered TBAs more aligned with local traditions as per the thematic analysis performed. Further delving into these barriers, a TBA woman revealed the pervasive fear and shame surrounding facility-based deliveries: “Women often fear to be known by others and feel ashamed about going to deliver at the clinic.” These narratives shed light on the intricate web of cultural beliefs and social dynamics shaping maternal healthcare decision-making. Moreover, the influence of family dynamics is palpable, as articulated by one participant: “My mother-in-law insisted I have the baby at home... and her opinion holds a lot of weight in our household.” These insights underscore the profound influence of sociocultural factors on healthcare-seeking behaviors.
Health facility-related factors that affect the utilization of skilled birth attendance
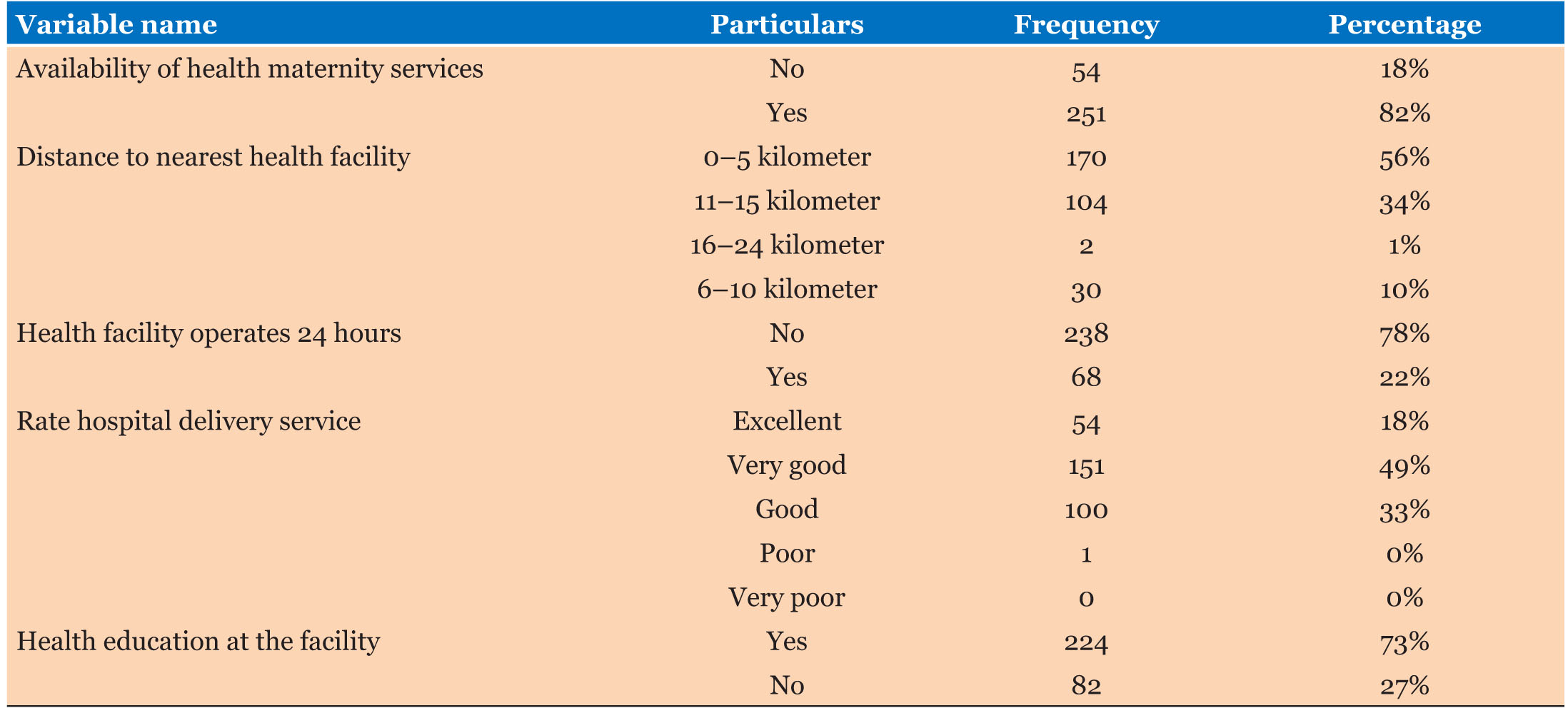
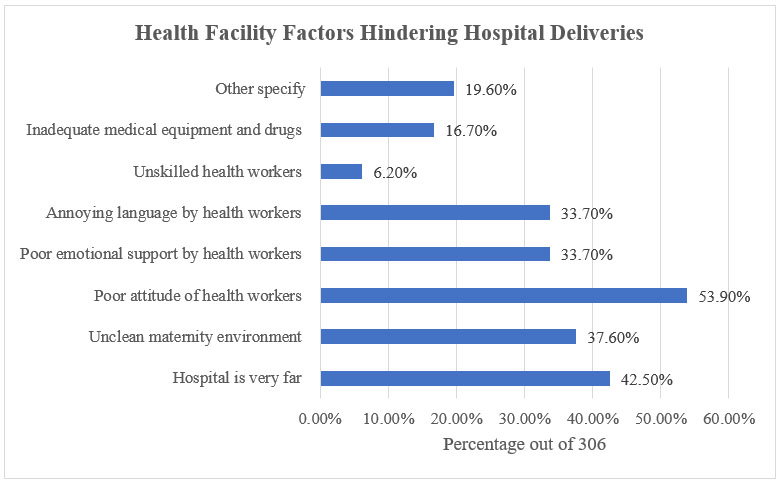
The data indicated most women (82% [n=251]) have a facility in their area providing maternity care. Proximity did not appear to be a universal barrier, as over half (56% [n=170]) of respondents had a facility within 5 km, with 34% (n=104) living 11–15 km away and some up to 24 km away. Also, most health centers were not open 24 hours (78% [n=238]). The majority described services as very good (49% [n=151]), followed by good at 33% (n=100). Commendably, 73% (n=224) of the participants stated that they received health education at the facility (Table 7). The data also highlighted several key barriers related to health facilities that deter women from seeking skilled delivery services. Distance was one major issue (42.5%), unsanitary maternity environments (37.6%), inadequate medical equipment/drugs (16.7%), negative healthcare worker attitudes (53.9%), insufficient emotional support (33.7%), and annoying language (33.7%) were reported as major barriers (Figure 1).
Further analysis explored health facility factors and their correlation with the place of delivery. The results underscored significant associations between health facility factors and delivery locations, with all factors showing statistical significance (p<0.001). Notably, the operation of public health facilities 24 hours, the proximity of hospitals, cleanliness of maternity environments, health worker attitudes, emotional support, language used by health workers, skill levels of health workers, and availability of medical equipment and drugs all exhibited significant relationships with the place of delivery selected by women (p<0.001). These findings emphasize the pivotal role of health facility factors in influencing maternal healthcare choices.
The qualitative analysis delved into the multifaceted health facility-related barriers impeding the adoption of skilled birth attendance. The thematic analysis revealed a landscape fraught with structural and capacity deficits within the healthcare system. The scarcity of dedicated maternal health establishments and trained personnel emerged as prominent themes. One CHV observed that the “unavailability of health facilities and few health workers here” were major barriers. Geographic inaccessibility also compounded these challenges. One community leader highlighted that “Distance from the facility means a 2-hour walk.” These barriers coalesced into two overarching themes: insufficient health infrastructure and workforce to serve dispersed villages, and vast distances to limited facilities. Participant testimonies vividly depicted the harsh realities of navigating these barriers, from enduring long journeys to attending understaffed facilities.
Discussion
This study delved into the multifaceted barriers influencing the utilization of skilled birth attendance (SBA) among women in North Horr ward, Marsabit County, Kenya. It drew from both quantitative data analysis and qualitative insights to present an in-depth analysis of the diverse factors that determine the choice of women on where they deliver their children. This study aligns findings with national maternal health statistics, revealing patterns in maternal age, marital status, parity, and education levels that impact maternal health-seeking behaviors [24],[25]. These demographic factors, particularly low education levels and economic constraints, emerged as significant barriers to accessing skilled birth attendance services [20]. Echoing research from South Asia and Ethiopia, addressing sociodemographic disparities can help improve maternal care utilization in developing countries [26],[27].
Transitioning to economic factors, the analysis underscores the pervasive influence of financial dependence, low incomes, and limited financial autonomy on women’s decision-making regarding childbirth [28],[29]. The study aligns with prior research, emphasizing the need for policy interventions such as health insurance subsidy programs and social protection initiatives to mitigate economic barriers and improve access to skilled birth attendance [30]. Sociocultural factors emerge as another critical determinant of maternal health-seeking behavior, with familial expectations, cultural norms, and trust in traditional birth attendants shaping women’s preferences for home births [3],[31]. Despite efforts to promote facility-based deliveries, deeply ingrained cultural traditions continue to influence women’s choices, underscoring the need for community engagement and sensitization approaches to shift societal perceptions [32] .
Lastly, health facility-related barriers are examined, revealing challenges related to distance, infrastructure, service quality, and health worker attitudes [16],[20],[33]. Despite geographic proximity to health facilities, deficiencies in staffing, resources, and quality of care undermine women’s confidence in facility-based deliveries [24]. The study recommends holistic health systems strengthening initiatives to address these barriers, including improvements in infrastructure, staffing, and interpersonal communication to ensure supportive and dignified skilled birth attendance experiences [20],[33]. Overall, the discussion underscores the interconnected nature of the barriers facing women in accessing skilled birth attendance, emphasizing the need for multifaceted interventions that address demographic, economic, sociocultural, and health facility-related factors to improve maternal health outcomes.
Conclusion
The study concludes that the barriers to utilizing skilled birth attendance services are multifaceted and deeply entrenched, encompassing economic, sociocultural, and health facility-related factors. It emphasizes the need for integrated interventions that address these challenges concurrently, requiring coordinated efforts from various stakeholders, including governments, non-governmental organizations (NGOs), and community leaders. Recommendations include targeted policy interventions to address poverty and infrastructure deficiencies, community engagement initiatives to shift cultural norms toward accepting skilled care, and strategic incorporation of unskilled attendants into formal health systems. However, it is acknowledged that no single solution can resolve these complex issues alone, necessitating sustained, long-term strategies that encompass access, infrastructure, quality of care, financing, and norms collectively over time through strategic integration. Additionally, future research directions include longitudinal analyses to evaluate the impact of interventions over time and expanded geographical diversity to validate findings across different settings. Overall, the study contributes valuable insights into the challenges surrounding skilled birth attendance and provides a foundation for developing effective strategies to improve maternal health outcomes in remote areas.
REFERENCES
1.
Gitobu CM, Gichangi PB, Mwanda WO. Satisfaction with delivery services offered under the free maternal healthcare policy in Kenyan public health facilities. J Environ Public Health 2018;2018:4902864. [CrossRef]
[Pubmed]

2.
Delivery care. UNICEF Data. 2018. [Available at: https://data.unicef.org/topic/maternal-health/delivery-care/]
3.
Moshi FV, Lymo G, Gibore NS, Kibusi SM. Prevalence and factors associated with home childbirth with unskilled birth assistance in Dodoma-Tanzania: A cross sectional study. East Afr Health Res J 2020;4(1):92–100. [CrossRef]
[Pubmed]
4.
A woman dies every two minutes due to pregnancy or childbirth: UN agencies. World Health Organization. 2023. [Available at: https://www.who.int/news/item/23-02-2023-a-woman-dies-every-two-minute-sdue-to-pregnancy-or-childbirth--un-agencies]
5.
Ngusie HS, Mengiste SA, Zemariam AB, et al. Predicting adverse birth outcome among childbearing women in Sub-Saharan Africa: Employing innovative machine learning techniques. BMC Public Health 2024;24(1):2029. [CrossRef]
[Pubmed]
6.
Newborn mortality. World Health Organization. 2021. [Available at: https://www.who.int/news-room/fact-sheets/detail/newborn-mortality]
7.
Gitobu CM, Gichangi PB, Mwanda WO. The effect of Kenya’s free maternal health care policy on the utilization of health facility delivery services and maternal and neonatal mortality in public health facilities. BMC Pregnancy Childbirth 2018;18(1):77. [CrossRef]
[Pubmed]
8.
Lang’at E, Mwanri L. Healthcare service providers’ and facility administrators’ perspectives of the free maternal healthcare services policy in Malindi District, Kenya: A qualitative study. Reprod Health 2015;12:59. [CrossRef]
[Pubmed]
9.
Njuguna J, Kamau N, Muruka C. Impact of free delivery policy on utilization of maternal health services in county referral hospitals in Kenya. BMC Health Serv Res 2017;17(1):429. [CrossRef]
[Pubmed]
10.
Orangi S, Kairu A, Ondera J, et al. Examining the implementation of the Linda Mama free maternity program in Kenya. Int J Health Plann Manage 2021;36(6):2277–96. [CrossRef]
[Pubmed]
11.
Masaba BB, Mmusi-Phetoe RM. Free maternal health care policy in Kenya; Level of utilization and barriers. Int J Afr Nurs Sci 2020;13:100234.
12.
Mathewos Oridanigo E, Kassa B. Utilization of skilled birth attendance among mothers who gave birth in the last 12 months in Kembata Tembaro Zone. Adv Med 2022;2022:8180387. [CrossRef]
[Pubmed]
13.
Mutinda MI. Factors Influencing Unskilled Delivery in Kenya. 2017. [Available at: http://erepository.uonbi.ac.ke/bitstream/handle/11295/103036/Mulinge_Factors%20Influencing%20Unskilled%20Delivery%20In%20Kenya.pdf?sequence=1]
14.
Bokayo Arero C, Margaret KN, Ayieko SY, Vincent MO, Geoffrey OM. Health system factors associated with choice of place of delivery among postnatal women in Marsabit County, Kenya. Int J Res Innov Soc Sci 2021;05(12):207–15.
15.
Latif AS. The importance of understanding social and cultural norms in delivering quality health care—A personal experience commentary. Trop Med Infect Dis 2020;5(1):22. [CrossRef]
[Pubmed]
16.
Moindi RO, Ngari MM, Nyambati VCS, Mbakaya C. Why mothers still deliver at home: Understanding factors associated with home deliveries and cultural practices in rural coastal Kenya, a cross-section study. BMC Public Health 2016;16:114. [CrossRef]
[Pubmed]
17.
Ansu-Mensah M, Danquah FI, Bawontuo V, et al. Quality of care in the free maternal healthcare era in sub-Saharan Africa: A scoping review of providers’ and managers’ perceptions. BMC Pregnancy Childbirth 2021;21(1):220. [CrossRef]
[Pubmed]
18.
Mutea L, Ontiri S, Kadiri F, Michielesen K, Gichangi P. Access to information and use of adolescent sexual reproductive health services: Qualitative exploration of barriers and facilitators in Kisumu and Kakamega, Kenya. PLoS One 2020;15(11):e0241985. [CrossRef]
[Pubmed]
19.
Duncan AC. Determinants of Skilled Delivery Services Utilization among Women of Reproductive Age in Migori County, Kenya. 2019. [Available at: https://ir-library.ku.ac.ke/server/api/core/bitstreams/155eafb3-4b8e-4878-9b67-5d187ccb690c/content]
20.
Kasaye HK, Endale ZM, Gudayu TW, Desta MS. Home delivery among antenatal care booked women in their last pregnancy and associated factors: Communitybased cross sectional study in Debremarkos Town, North West Ethiopia, January 2016. BMC Pregnancy Childbirth 2017;17(1):225. [CrossRef]
[Pubmed]
21.
Green EC, Murphy EM, Gryboski K. The health belief model. Wiley Encycl Health Psychol 2020;1(1):211–4.
22.
Shieh G. Optimal sample sizes for the design of reliability studies: Power consideration. Behav Res Methods 2014;46(3):772–85. [CrossRef]
[Pubmed]
23.
Boddy CR. Sample size for qualitative research. Qualitative Market Research: An International Journal 2016;19(4):426–32. [CrossRef]
24.
Maternal, Infant and Young Children Nutrition Knowledge Attitude and Practices Baseline Survey for Marsabit County. 2018. [Available at: https://www.nutritionhealth.or.ke/wp-content/uploads/MIYCN%20Assessments%20Reports/Marsabit%20County%20MIYCN%20KAP%20Report%20-%20January%202018.pdf]
25.
Muheirwe F, Nuhu S. Are health care facilities and programs in Western Uganda encouraging or discouraging men’s participation in maternal and child health care? Int J Health Plann Manage 2019;34(1):263–76. [CrossRef]
[Pubmed]
26.
Abadiga IT, Tereda AB. Utilization of skilled birth attendant in Bonga Town, Kafa Zone, South West Ethiopia. Gynecol Obstet (Sunnyvale) 2016;6(9):402. [CrossRef]
27.
Rodamo KM, Salgedo WB, Nebeb GT. Magnitude and determinants of utilization of skilled birth attendance among women of child bearing age in Sidama Zone, Southeast Ethiopia. Gynecol Obstet (Sunnyvale) 2015;5(6):300. [CrossRef]
28.
Simel LL, Nanduri L, Juma PA, Omuga B. An evaluation of economic and education determinants on utilization of skilled delivery services by Maasai Women in Kiekonyokie sub location of Kajiado County in Kenya. Int J Community Med Public Health 2018;5(2):437–42.
29.
Nyongesa C, Xu X, Hall JJ, Macharia WM, Yego F, Hall B. Factors influencing choice of skilled birth attendance at ANC: Evidence from the Kenya demographic health survey. BMC Pregnancy Childbirth 2018;18(1):88. [CrossRef]
[Pubmed]
30.
Mutuku J, Githae DM. Delays in Africa accessing emergency obstetric care in sub-saharan; Kenya situation. International Journal of Contemporary Research and Review 2018;9(7):20484–96. [CrossRef]
31.
Garces A, McClure EM, Espinoza L, et al. Traditional birth attendants and birth outcomes in low-middle income countries: A review. Semin Perinatol 2019;43(5):247–51. [CrossRef]
[Pubmed]
32.
Manyiwa JS, Kamiruka J, Yuko OW. The role of organized public forums in improving uptake of skilled birth attendants among women of reproductive age in Kilifi County, Kenya. Texila International Journal of Public Health 2023;11(1):245–52. [CrossRef]
33.
Mekonnen T, Dune T, Perz J. Maternal health service utilisation of adolescent women in sub-Saharan Africa: A systematic scoping review. BMC Pregnancy Childbirth 2019;19(1):366. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Kame Wato Kofo - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Micah Matiang’i - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maureen Akolo - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Kame Wato Kofo et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}