 |
Research Article
Factors associated with preconception care practices among women visiting Mother and Child Health Clinic in Nakuru County Referral and Teaching Hospital, Kenya: A mixed-methods study
1 Department of Community Health, School of Public Health, Amref International University (AMIU), Nairobi, Kenya
2 Lecturer, Department of Community Health, School of Public Health, Amref International University (AMIU), Nairobi, Kenya
3 Lecturer and Consultant Nutritionist, Department of Health Sciences, School of Agriculture, Environment and Health Sciences, Machakos University, Machakos, Kenya
Address correspondence to:
Lucky Oseghale Oloboh
Department of Community Health, School of Public Health, Amref International University (AMIU), Nairobi,
Kenya
Message to Corresponding Author
Article ID: 100014M01LO2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Oloboh LO, Kuria-Ndiritu S, Muia-Matuku EN. Factors associated with preconception care practices among women visiting Mother and Child Health Clinic in Nakuru County Referral and Teaching Hospital, Kenya: A mixed-methods study. Edorium J Matern Child Health 2025;8(1):1–11.ABSTRACT
Aims: Despite the recognized importance of preconception care (PCC) to enhance maternal and fetal health, there is limited understanding of the factors affecting its uptake, especially in diverse socio-economic and cultural contexts. This study aimed to evaluate the level of PCC practices, explore socio-demographic factors influencing PCC utilization, examine the relationship between PCC knowledge and practices, and identify factors affecting PCC adherence among women attending the Mother and Child Health Clinic at Nakuru County Referral and Teaching Hospital, Kenya.
Methods: A descriptive cross-sectional study utilizing a mixed-methods approach was conducted. Quantitative data were collected from 436 women aged 18–49 via simple random sampling using structured and semi-structured questionnaires. Data were analyzed using SPSS version 26.0, with univariate and bivariate analyses to identify significant associations (p<0.05). Qualitative 2025 data were gathered through focus group discussions and analyzed thematically to contextualize findings.
Results: Among respondents, PCC practice levels were high: 87% reported folic acid use, 68% took iron supplements, 63% received nutritional counseling, and 61% obtained preconception vaccinations [e.g., Rubella, Hepatitis B, Influenza, and human papillomavirus (HPV)]. Knowledge of PCC was moderate at 69%. Significant associations were found between PCC practices and socio-demographic factors, including age, education, occupation, and monthly income (p<0.001). Preconception care knowledge also significantly impacted practices. Additional factors influencing PCC adherence included cultural beliefs, previous obstetric complications, and partner support.
Conclusion: Preconception care practices are influenced by socio-demographic and socio-economic factors, alongside cultural beliefs and support systems. Addressing these determinants through targeted interventions and continued stakeholder engagement is critical for improving PCC uptake and ensuring better maternal and fetal outcomes in Nakuru County.
Keywords: Kenya, Nakuru, Preconception care practices, Women of reproductive age
Introduction
Preconception care (PCC) is a proactive intervention designed to identify and address biomedical, behavioral, and social factors that could adversely impact pregnancy outcomes and long-term maternal and child health. Its goal is to promote healthier pregnancies by optimizing women’s health before conception [1],[2]. Although the concept of PCC can be traced back to early medical literature, such as Dewees’ 1858 advocacy for pre-marital health assessments, it remains highly relevant today. The Centers for Disease Control and Prevention (CDC) defines PCC as a series of health interventions aimed at improving reproductive health through measures such as promoting healthy lifestyles, managing pre-existing conditions, preventing infectious diseases, and ensuring adequate vaccination coverage (CDC, 2020) [3].
Despite its proven benefits, the global uptake of PCC remains suboptimal. For example, PCC practices among diabetes-affected patients range between 18.7% and 45% in Canada, approximately 45% in England, and between 33% and 47.7% in the United States [4]. The uptake is even lower in Sub-Saharan Africa (SSA), where maternal and neonatal health outcomes are among the poorest globally. In 2017, the maternal mortality ratio in SSA was 211 per 100,000 live births, with 66% of global maternal deaths occurring in this region [5]. Contributing factors include limited awareness of PCC, inadequate access to healthcare services, and socio-cultural barriers. Studies report that only 11% of women in Sudan, 15.4% in Nepal, and 38.3% in Kenya are aware of PCC [6].
In Kenya, maternal mortality remains a significant public health concern, with Nakuru County recording a high maternal mortality ratio of 374 per 100,000 live births, ranking fourth in the country [7]. Adolescent pregnancies and the low uptake of maternal and reproductive health services significantly contribute to maternal mortality in Kenya. A study by Wambui et al. highlights that adolescent pregnancy and complications during childbirth are major contributors to mortality among adolescents and young women [8]. While previous studies have explored PCC utilization in various parts of Kenya, gaps remain in understanding the factors influencing PCC practices in referral and teaching hospitals, particularly in Nakuru County. Research conducted in similar settings has shown that socio-economic factors, education levels, cultural beliefs, and healthcare accessibility are critical determinants of PCC uptake [9],[10].
Given the high maternal mortality rates and limited awareness of PCC practices in Nakuru County, there is an urgent need to investigate the socio-demographic, economic, and cultural factors influencing PCC uptake. This study focuses on assessing these factors among women attending Maternal and Child Health (MCH) clinics at the Nakuru County Referral and Teaching Hospital (NCRTH). The findings aim to inform strategies for improving PCC awareness and utilization, ultimately contributing to better maternal and fetal health outcomes in the region.
Operationalization of preconception care practices
Implementing preconception care (PCC) practices requires adherence to established health guidelines and recommendations. This includes actively seeking timely and comprehensive PCC services, following professional medical advice, and making informed decisions based on a clear understanding of PCC principles and benefits.
This study is guided by the Health Belief Model (HBM), which posits that individuals’ health behaviors are shaped by their perceptions of health risks and the effectiveness of preventive measures [11]. Within this framework, women are more likely to engage in PCC when they recognize a significant risk of pregnancy complications and believe that PCC practices can effectively mitigate these risks. The HBM further suggests that the decision to adopt PCC practices is driven by a cost–benefit analysis, where perceived benefits must outweigh perceived barriers for meaningful behavior change to occur.
Independent variables
Socio-demographic factors
Aspects of socio-demographic factors tested included age, marital status, number of children, religion, educational status, occupation, monthly income, and source of information.
Knowledge of preconception care
The study tested the following dimensions: knowledge of folic acid and iron supplementations, avoidance of teratogenic substances, awareness of the benefits of preconception counseling, etc.
Factors associated with preconception care practices
The following aspects of preconception care services were tested: accessibility, availability, and affordability.
Dependent variable
Preconception care practices
For preconception care practices, the following aspects were tested: seeking counseling from healthcare providers, undergoing essential screenings, maintaining a healthy weight, quitting smoking, managing chronic conditions, and starting folic acid and iron supplements at least one month before pregnancy.
MATERIALS AND METHODS
Research design
A cross-sectional design with a mixed-methods approach was utilized. Quantitative data were gathered using interviewer-administered structured and semi-structured questionnaires, which provided a broad overview of PCC practices among women. Complementing this, qualitative data were collected through focus group discussions (FGDs).
Study site
The study was conducted at NCRTH, located in Nakuru City, Kenya. Nakuru is Kenya’s fourth-largest city; approximately 160 km west of Nairobi along the Trans-African Highway. Nakuru County Referral and Teaching Hospital serves as the central referral hospital for Nakuru County and the environs with a projected population of 7 million. With a capacity of 600 beds, the NCRTH serves a diverse population of approximately 3.6 million residents, including patients from neighboring environs such as Central, Western, and Nyanza Kenya. Additionally, it plays a pivotal role as a teaching facility for local health training institutions, including the Schools of Medicine at Kabarak and Egerton Universities. The hospital provides comprehensive health services, including curative, rehabilitative, promotive, and preventive care. Nakuru County Referral and Teaching Hospital was chosen for this study due to its significant role in managing maternal health, particularly given Nakuru County’s high maternal mortality rate of 374 per 100,000 live births.
Study population and target population
Preconception care utilization refers to any healthcare engagement by women of reproductive age with healthcare providers aimed at addressing pregnancy planning, preparation, and health optimization before conception. The study population included women who had lived in Nakuru for at least six months and had accessed reproductive health services at NCRTH. Women aged 18–49 years with a focus on those who visited the MCH clinics at NCRTH during the study period were the target population.
A sample size of 436 women was calculated using Slovin’s formula and adjusted for non-responses. The women were selected through stratified random sampling within each clinic and simple random sampling within each stratum. Reaching saturation, eight focus group discussions were conducted for qualitative data collection, each with 6–8 participants from the different MCH clinics to ensure diverse perspectives. Focus group discussions were held with women from varying socio-economic backgrounds and geographic locations within Nakuru. The study focused on women already engaged with MCH services due to the socio-cultural challenges in identifying those planning pregnancies; information on the care they received before their current or most recent pregnancy was sought. Annually, about 39,446 women seek services at NCRTH’s MCH clinics, distributed across the antenatal (14,183), child welfare (15,647), postnatal (4,743), and family planning (4,873) clinics (Records and Registry data, 2023).
Data collection instruments
Data collection instruments comprised interviewer-administered structured and semi-structured questionnaires for quantitative data and focus group discussion (FGD) guides for qualitative data. The questionnaires were administered via Google Forms and respondents were selected through simple random sampling. Using Excel to generate random numbers for each respondent in the sampling frame, samples with the numbers in the respective MCH clinics at NCRTH were selected for the study’s data collection. Qualitative data were collected through FGD guides facilitating discussions on the women’s personal opinions and experiences to saturation; thus, complementing the quantitative findings.
Data analysis
Data were sorted, coded, and analyzed using SPSS version 26.0, with a significance level set at 95% (p-value < 0.05). Univariate analysis was conducted to evaluate descriptive variables, while bivariate analysis employed chi-square tests to assess associations between dependent and independent variables. Results were presented through descriptive statistics, and qualitative data were analyzed thematically, enriching the discussions within the findings.
Ethical considerations
Ethical approval was obtained from relevant authorities which included approval from the Amref Health Africa Ethics and Scientific Review Committee (ESRC P1388/2023) and the National Commission for Science, Technology and Innovation (NACOSTI/P/23/25780). Informed consent was sought from all respondents and measures were implemented to ensure respondents’ voluntary participation, privacy, and confidentiality.
RESULTS
In this study, 436 women seeking reproductive health services were recruited across four clinic settings: 157 from the antenatal clinic, 173 from the child welfare clinic, 52 from the postnatal clinic, and 54 from the family planning clinic. The study achieved a 100% response rate, surpassing the thresholds suggested by Sammut et al. [12] for acceptable (50%), good (60%), and very good (70%) response rates.
Respondents’ socio-demographic association with preconception care practices
The researchers found that 77% of the women were Christians, with 54% having attained college-level education or higher. Marital status was diverse, with 47% being married. Most women (42%) earned between 10,001 and 16,999 Ksh. monthly, and 38% were primigravida. Occupation-wise, 38% were civil servants, and 34% were aged 26–33 years. A chi-square analysis revealed significant associations between preconception care practices and several socio-demographic factors: age (χ2=374.443, p<0.001), education (χ2=384.288, p<0.001), occupation (χ2=268.305, p<0.001), and income (χ2=229.288, p<0.001) (Table 1).
Respondents’ knowledge level association with preconception care practices
Among the 436 women surveyed, 69% had heard of preconception care, while 31% had not. Of those aware of PCC, 56% knew its key components, such as immunization updates, healthy diet and micronutrient supplementation, chronic disease management, family planning, and avoiding substance abuse, while 44% lacked this knowledge. Key aspects of PCC knowledge included the importance of folic acid and iron supplements, avoidance of teratogenic substances, and seeking preconception counseling. Women identified various negative outcomes of neglecting PCC practices, including miscarriage, birth defects, low birth weight, stillbirth, anemia, etc. Despite this, only 51% of these women reported starting iron-folic acid supplementation (IFAS) at least one month before pregnancy. Chi-square analyses revealed significant associations between both general knowledge of PCC (χ2=109.29, p<0.001) and knowledge of its components (χ2=163.982, p<0.001) with the practice of preconception care (Table 2).
Respondents’ level of preconception care practices
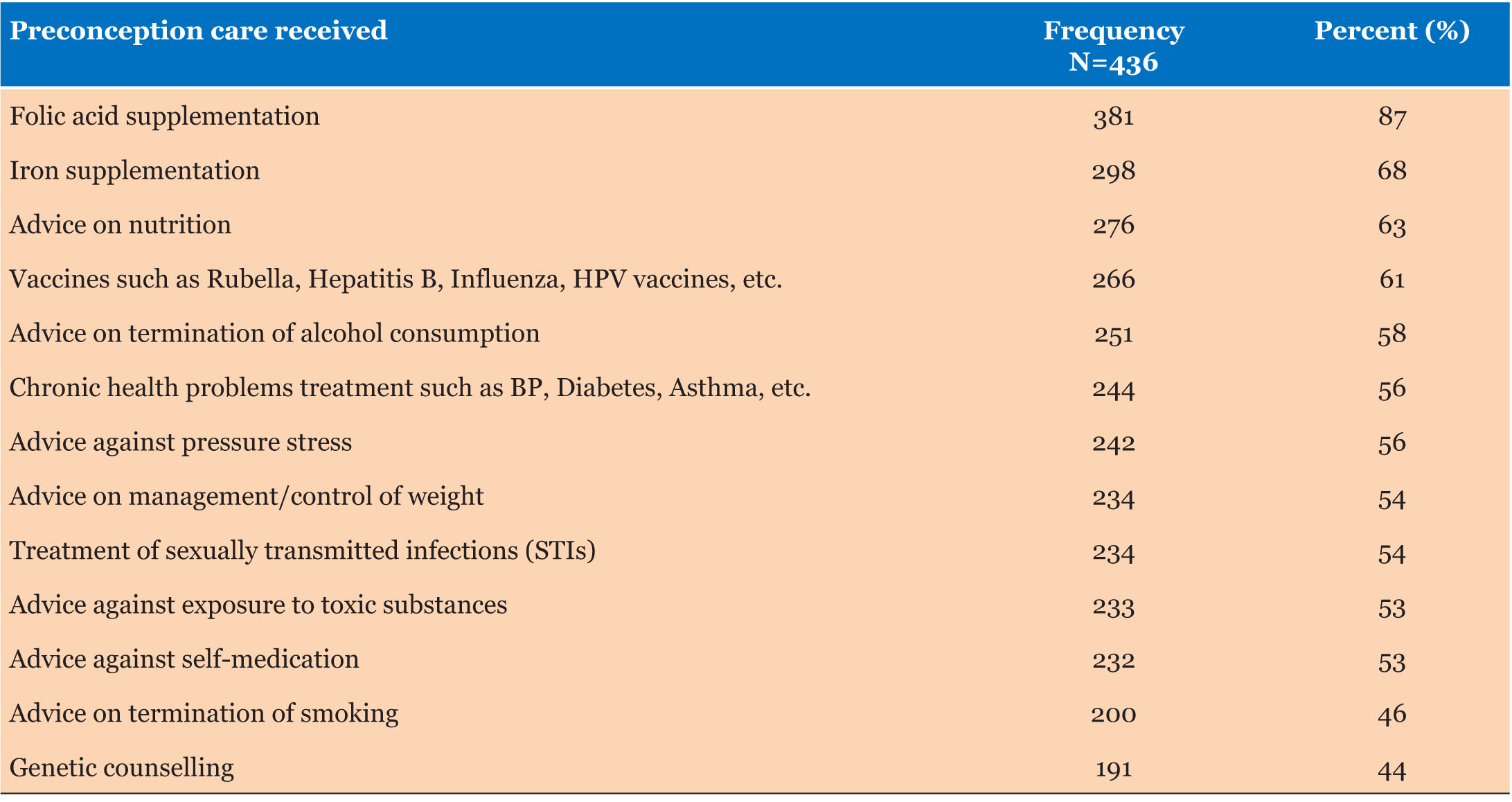
The researchers assessed PCC practices by evaluating the women’s adherence to established PCC principles. This includes seeking timely services, following healthcare recommendations, and making informed decisions based on PCC knowledge. Proper PCC practices involved engaging in behaviors aligned with these guidelines, while improper practices reflected deviations from recommended behaviors, such as inadequate knowledge or neglecting necessary healthcare. Results indicated that 65% of women reported their last/current pregnancy was planned notwithstanding the high PCC practice findings. As a study limitation, some mothers might have misunderstood and confused preconception care and antenatal care while answering the questions in the questionnaire or they might have answered according to what they know is right rather than the actual PCC practice. The study design does not confirm causation; thus, there might have been reporting bias. Among the PCC services received, folic acid supplementation was the most common (87%), followed by iron supplementation (68%), nutrition advice (63%), and vaccination (61%). Genetic counseling was the least received service, reported by 44% of women (Table 3).
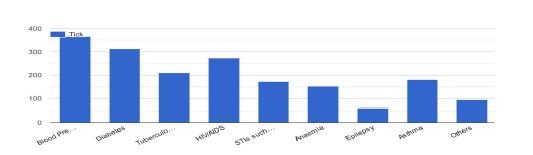
Regarding their medical screening, 78% of the women reported being screened for several medical conditions before conception, while 22% had not. The most commonly screened conditions were high blood pressure (84%), diabetes (72%), and human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) (63%). Less frequently screened conditions included tuberculosis (48%), asthma (41%), and sexually transmitted infections (STIs) (40%), with anemia and epilepsy being the least screened (35% and 14%, respectively) (Figure 1).
Factors influencing respondents’ preconception care practices
We, as researchers, identified several factors significantly associated with preconception care practices. Age was a key factor, with women aged 25 and above more likely to engage in PCC compared to those under 25 (χ2=374.443, p<0.001). Educational status also played a role, as women with higher education levels were more likely to practice PCC than those with no formal or only primary education (χ2=384.288, p<0.001). Employment status further influenced PCC practices, with employed women more likely to engage in PCC compared to unemployed women (χ2=268.305, p<0.001). Lastly, monthly income was associated with PCC practices, indicating that women with higher incomes were more likely to practice PCC than those with lower or no income (χ2=229.288, p<0.001).
Chi-square tests revealed significant associations between both the overall knowledge of preconception care (χ2=109.29, p<0.001) and specific knowledge of PCC components (χ2=163.982, p<0.001) with PCC practices. These findings underscore that while knowledge provides the theoretical foundation necessary for effective PCC, practical application is crucial for realizing the benefits of that knowledge. Effective PCC practice requires not only knowledge comprehension but also knowledge application; a balance between the two ensures that theoretical insights are translated into meaningful actions. This balance is essential for achieving successful PCC outcomes among women attending the MCH clinic in NCRTH.
The impact of cultural beliefs and misconceptions on preconception care practices was assessed by the researchers. 24% of women reported that cultural factors influenced their PCC practices, while 76% did not perceive such a relationship. Chi-square analysis revealed a significant association between preconception-related cultural beliefs and misconceptions and PCC practices (χ2=293.009, p<0.001). Notable misconceptions included fears of miscarriage from sharing pregnancy intentions, beliefs that engaging in PCC could hinder pregnancy, and concerns about becoming impotent from medication and vaccines.
Previous obstetric complications impact on preconception care practices was explored by the researchers. Among the women surveyed, 88% had not experienced any obstetric complications in previous pregnancies, while 12% had experienced issues such as miscarriages (5%), stillbirths (3%), prolonged labor (3%), or preeclampsia (1%). Of the 169 women who responded about the influence of past-complications on PCC practices, 56% believed their experiences affected their PCC practices, whereas 44% did not. Significant associations were found between the occurrence of previous obstetric complications and PCC practices (χ2=26.994, p<0.001), and between the influence of these complications on PCC practices (χ2=360.345, p<0.001).
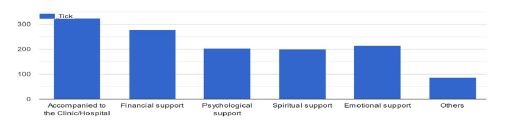
The researchers also examined how partner support during the preconception period affects preconception care practices. Women of reproductive age who were accompanied to clinics or hospitals by their partners during the study reported receiving the highest level of support during the preconception period. In contrast, psychological and spiritual support was less commonly received by these women (Figure 2).


Discussion
This study employs quantitative and qualitative methods to assess factors influencing preconception care practices among women at MCH Clinics in NCRTH, Kenya. It determines socio-demographic factors with PCC practices, knowledge levels, and overall engagement with PCC. According to our study, women who were older, better educated, employed, and had higher incomes were more likely to engage in regular PCC. These results align with previous research by Chepngetich [13], Demisse et al. [14], and Olayinka et al. [15], which indicates that women who seek preconception care are more likely to be over 25 years old, highly educated, employed, and have higher incomes. These studies suggest that higher education and stable employment increase exposure to PCC information and utilization. Thus, lower educational status is linked to reduced exposure to preconception care information [13],[14],[16]. Additionally, employed women tend to practice PCC more frequently than their unemployed counterparts, which could be attributed to their greater resources and health-seeking behaviors. However, this finding contrasts with a Nigerian study [15], which found no significant link between occupation and maternal healthcare use, possibly due to the availability of free reproductive healthcare services in Nigeria that may mitigate the impact of employment status. Overall, the study underscores the significant role of socio-demographic factors in PCC practices and the necessity for targeted educational and support interventions to address disparities in PCC utilization across various socio-economic groups.
A significant link between knowledge about preconception care and actual PCC practices was noticed by the researchers. Women knowledgeable of PCC’s components and their benefits are more likely to engage in PCC practices; highlighting the critical role of educational interventions in enhancing PCC uptake. Approximately 70% of women at the MCH clinics in NCRTH were aware of PCC, including its purpose, components, and associated risks. Focus group discussions reinforced that effective PCC involves understanding and applying medical advice for a healthy pregnancy. This underscores the necessity of promoting PCC knowledge to foster healthy practices and improve pregnancy outcomes [17],[18],[19]. The researchers noted that 91% of women were aware of iron-folic acid supplementation (IFAS), which is recommended to begin 1–3 months before conception to ensure adequate nutrient levels for fetal development and maternal health. Despite this, only 51% of women reported starting IFAS at least one month before pregnancy. This study found a high level of preconception care knowledge among women at NCRTH, contrasting with the lower levels reported in other Kenyan studies. This disparity may be due to socio-demographic factors such as higher education, age, and income in the NCRTH sample. The greater PCC awareness observed in this study aligns with findings from research in the United States [20],[21] and supports the link between higher education and increased use of maternal health services [22]. This contrasts with sub-Saharan African studies, which have reported suboptimal PCC knowledge [13],[16],[17],[18],[23],[24],[25], possibly due to different settings and sample characteristics. Overall, the study emphasizes the importance of integrating knowledge with practice in PCC and the influence of socio-demographic factors on PCC awareness and utilization.
Many women in MCH clinics at NCRTH actively engaged in PCC practices, such as pregnancy planning and early care, and using services such as folic acid and iron supplementation, nutritional advice, vaccination, and genetic counseling. Over half of the women also underwent screening for conditions like high blood pressure, diabetes, HIV/AIDS, and tuberculosis, indicating robust PCC engagement within this cohort. This high level of PCC practice is consistent with previous research showing that older, highly educated, employed, and higher-income women are more likely to utilize and adhere to PCC [13],[14],[15]. The study’s findings align with the Health Belief Model (HBM), which posits that personal beliefs and awareness significantly drive health-seeking behaviors [11]. The elevated preconception care practices at NCRTH compared to other Kenyan studies [9],[13],[22] may be attributed to higher socio-demographic factors, such as education and income levels among the NCRTH population. This reinforces the trend that education, employment status, and income positively influence the use of maternal health services [22].
Despite the strong preconception care practices demonstrated among women in MCH clinics at NCRTH, notable gaps were also identified. While many women engaged in various PCC activities, such as screening for major conditions and using folic acid and iron, there was a lower record of family planning methods utilization before conception. Thus, as a study limitation, some mothers might have misunderstood and confused preconception care and antenatal care while answering the questions or they might have answered according to what they know is right rather than the actual practice; the study design does not confirm causation, so there might have been reporting bias. This finding is consistent with other sub-Saharan studies highlighting the underutilization of family planning; possibly due to the region lacking adequate knowledge of reproductive life planning concepts [25]. Additionally, the higher use of folic acid at NCRTH compared to some Kenyan and Ethiopian studies [13],[17],[18] may reflect regional differences in awareness and availability. The study also noted that while screenings for conditions like blood pressure and HIV/AIDS were common, screenings for conditions such as asthma, STIs, anemia, and epilepsy were less frequent. Thus, suggesting a focus on certain health issues while others are overlooked, potentially due to healthcare providers’ priorities and resource allocation variations. Overall, the study highlights that, although PCC practices at NCRTH are high and influenced by educational and socio-economic factors, there are gaps, particularly in family planning and comprehensive PCC coverage. Addressing these gaps requires more consistent and holistic PCC approaches, ensuring better integration of all recommended components and reducing practice disparities.
The importance of contextual factors in shaping PCC knowledge and practices is highlighted by the study results. It underscores the need for targeted educational interventions in diverse settings, especially in rural and less-resourced areas, to address knowledge gaps and improve PCC practices across different populations. This study reveals a strong link between the level of knowledge about PCC and actual PCC practices, with higher knowledge levels correlating significantly with increased engagement in these practices. This finding contrasts with previous research in sub-Saharan Africa, which often reports lower PCC knowledge and its adverse impact on PCC practices [13],[16],[17],[18],[23],[24],[25]. The observed discrepancy may be attributed to the study’s setting, an urban referral and teaching hospital, which likely offers a more structured educational environment compared to the varied urban and rural settings of other studies. This setting potentially provides more consistent and comprehensive PCC information, enhancing knowledge and practices. In contrast, rural and semi-urban areas may face challenges such as limited healthcare infrastructure and lower educational outreach, affecting PCC knowledge and utilization. Differences in sample sizes and study methodologies also contribute to these variations. The urban setting of this study might show more localized educational impacts, while broader trends could emerge from larger and more diverse samples across various settings.
This study identifies a significant association between cultural factors and preconception care practices, emphasizing the profound impact of culture on how PCC is approached and perceived. This finding extends Kang’s [26] research, which highlighted cultural influences on birth and perinatal care, by demonstrating that cultural factors also critically shape PCC practices. The strong chi-square value indicates a robust link between cultural variations and PCC practices, highlighting the importance of incorporating cultural considerations into PCC strategies. The study underscores cultural beliefs such as fears of infertility or miscarriage linked to sharing pregnancy intentions, and concerns about the side effects of medicines and vaccines can significantly affect women’s engagement with PCC. These cultural barriers revealed through focus group discussions suggest that a one-size-fits-all approach to PCC may not be effective. Aligning with Kang’s insights, the study reinforces the necessity of integrating cultural competence into PCC frameworks. To enhance patient outcomes, healthcare providers should tailor PCC approaches to align with cultural contexts. This includes embedding cultural awareness into professional training and PCC strategies, ensuring that care is both patient-centered and culturally sensitive. Addressing these cultural factors can improve the effectiveness and responsiveness of PCC, leading to better patient engagement and outcomes.
Partner support plays a significant role in influencing preconception care practices. Key forms of support identified in this study include accompaniment to clinic or hospital visits and financial assistance. Women who reported having received such support from their partners reported increased motivation and engagement with PCC. Focus group discussions further emphasized that, although women are ultimately responsible for their clinic visits, the presence and backing of their partners, both emotionally and financially, serve as major motivators for practicing PCC. These findings are consistent with Stephenson et al.’s [27] research, which underscores the critical role of partner involvement in enhancing women’s engagement with PCC. The study highlights that effective PCC practices are significantly supported by partners, suggesting that fostering strong support systems can improve PCC adherence and outcomes.
A significant relationship between previous obstetric complications and increased engagement in preconception care practices was noted in the study results. Women with a history of obstetric complications showed a higher likelihood of seeking PCC, as evidenced by significant associations (χ2=26.994, p<0.001) and (χ2=360.345, p<0.001). These findings indicate that past experiences with obstetric complications strongly influence women to proactively pursue PCC to mitigate future risks. This outcome aligns with Chuang et al.’s [28] research, which found that women with chronic conditions are motivated to adopt proactive health measures before subsequent pregnancies. The study underscores that personal medical history, especially past complications, significantly impacts women’s commitment to PCC, highlighting the importance of addressing these experiences to enhance preconception health behaviors.
Conclusion
The researchers assessed factors influencing preconception care practices among women at the Nakuru County Referral and Teaching Hospital in Kenya. Key findings indicated that women at NCRTH generally possess a strong understanding of PCC services and engage extensively in practices. The study identified several factors affecting PCC practices; thus, recommends increased awareness and preventive visits across all life stages, integrating comprehensive counseling services for women; and ongoing support and education by the Nakuru County government and stakeholders to sustain and enhance PCC knowledge and practice. Also, to reinforce the importance of family planning as a key component of PCC during women’s health visits, healthcare providers should work to correct cultural misconceptions about PCC to improve understanding and acceptance. Future research direction to focus on assessing the quality of preconception care practices to gain deeper insights into and enhance the effectiveness of PCC. Overall, the study underscores the importance of sustained educational efforts, socio-demographic considerations, and cultural sensitivity in improving preconception care practices.
REFERENCES
1.
Ojifinni OO, Ibisomi L. Preconception care practices in Nigeria: A descriptive qualitative study. Reprod Health 2020;17(1):172.
[Pubmed]

2.
Suto M, Mitsunaga H, Honda Y, Maeda E, Ota E, Arata N. Development of a health literacy scale for preconception care: A study of the reproductive age population in Japan. BMC Public Health 2021;21(1):2057. [CrossRef]
[Pubmed]
3.
Atrash H, Jack B. Preconception care: Developing and implementing regional and national programs. J Hum Growth Dev 2020;30(3):398–406.
4.
Morema EN, Senghor M, Ouma C. Prevalence of preconception care provision in Kisumu county-Kenya. MedRxiv 2022.
5.
Abayneh H, Wakgari N, Ganfure G, Bulto GA. Knowledge, attitude, and practice of preconception care and associated factors among obstetric care providers working in public health facilities of West Shoa Zone, Ethiopia: A cross-sectional study. PLoS One 2022;17(8):e0272316. [CrossRef]
[Pubmed]
6.
Lemma T, Silesh M, Taye BT. Knowledge of preconception care among reproductive-age women in Debre Berhan Town, Ethiopia: A community-based, cross-sectional study. BMJ Open 2022;12(5):e053855. [CrossRef]
[Pubmed]
7.
Nyachwaya NS, Mwanzo I, Osur J. Predictors of unsafe abortion among women seeking postabortion care at the Nakuru County Referral Hospital, Nakuru County Kenya. International Academic Journal of Health, Medicine and Nursing 2023;2(1):292–313.
8.
Wambui T, Obonyo B, Wanzala P. Adolescent pregnancy and challenges in Kenyan context. Journal of Global Health Perspectives 2018;3(1):45–52.
9.
Wanyonyi MK, Abwalaba RA. Awareness and beliefs on preconception health care among women attending maternal & child health services at Moi Teaching and Referral Hospital in Eldoret, Kenya. Journal of Health, Medicine and Nursing 2019;60. [CrossRef]
10.
Oketch DA, Onguru DD, Ogolla DS, Andrew G. Factors influencing preconception care services among women of reproductive age at Jaramogi Oginga Odinga Teaching and Referral Hospital, Kisumu. World Journal of Innovative Research 2021;10(4):82–94.
11.
Wegene MA, Gejo NG, Bedecha DY, Kerbo AA, Hagisso SN, Damtew SA. Utilization of preconception care and associated factors in Hosanna Town, Southern Ethiopia. PLoS One 2022;17(1):e0261895. [CrossRef]
[Pubmed]
12.
Sammut R, Griscti O, Norman IJ. Strategies to improve response rates to web surveys: A literature review. Int J Nurs Stud 2021;123:104058. [CrossRef]
[Pubmed]
13.
Chepngetich J. Utilization of preconception care services among women of reproductive age in Kiambu County, Kenya [Thesis, Kenyatta University]. 2018. [Available at: https://ir-library.ku.ac.ke/handle/123456789/18676]
14.
Demisse TL, Aliyu SA, Kitila SB, Tafesse TT, Gelaw KA, Zerihun MS. Utilization of preconception care and associated factors among reproductive age group women in Debre Birhan town, North Shewa, Ethiopia. Reprod Health 2019;16(1):96. [CrossRef]
[Pubmed]
15.
Olayinka OA, Achi OT, Amos AO, Chiedu EM. Awareness and barriers to utilization of maternal health care services among reproductive women in Amassoma community, Bayelsa State. Int J Nurs Midwifery 2014;6(1):10–5.
16.
Umar AG, Nasir S, Tunau K, Singh S, Ibrahim UA, Hassan M. Awareness and perception of preconception care among women in Usmanu Danfodiyo University Teaching Hospital Sokoto, North-Western Nigeria. J Family Med Prim Care 2019;8(5):1696–700. [CrossRef]
[Pubmed]
17.
Teshome F, Kebede Y, Abamecha F, Birhanu Z. What do women know before getting pregnant? Knowledge of preconception care and associated factors among pregnant women in Mana district, Southwest Ethiopia: A community-based cross-sectional study. BMJ Open 2020;10(7):e035937. [CrossRef]
[Pubmed]
18.
Teshome F, Kebede Y, Abamecha F, Birhanu Z. Why do women not prepare for pregnancy? Exploring women’s and health care providers’ views on barriers to uptake of preconception care in Mana District, Southwest Ethiopia: A qualitative study. BMC Pregnancy Childbirth 2020;20(1):504. [CrossRef]
[Pubmed]
19.
Dowell LJ. The relationship between knowledge and practice. The Journal of Educational Research 1969;62(5):201–5.
20.
Coonrod DV, Bruce NC, Malcolm TD, Drachman D, Frey KA. Knowledge and attitudes regarding preconception care in a predominantly low-income Mexican American population. Am J Obstet Gynecol 2009;200(6):686.e1–7. [CrossRef]
[Pubmed]
21.
Frey KA, Files JA. Preconception healthcare: What women know and believe. Matern Child Health J 2006;10(5 Suppl):S73–7. [CrossRef]
[Pubmed]
22.
Okemo JK, Kamya D, Mwaniki AM, Temmerman M. Determinants of preconception care among pregnant women in an urban and a rural health facility in Kenya: A qualitative study. BMC Pregnancy Childbirth 2021;21(1):752. [CrossRef]
[Pubmed]
23.
Okemo J, Temmerman M, Mwaniki M, Kamya D. Preconception care among pregnant women in an urban and a rural health facility in Kenya: A quantitative study. Int J Environ Res Public Health 2020;17(20):7430. [CrossRef]
[Pubmed]
24.
Ayalew Y, Mulat A, Dile M, Simegn A. Women’s knowledge and associated factors in preconception care in Adet, West Gojjam, Northwest Ethiopia: A community based cross sectional study. Reprod Health 2017;14(1):15. [CrossRef]
[Pubmed]
25.
Ukoha WC, Mtshali NG, Adepeju L. Current state of preconception care in sub-Saharan Africa: A systematic scoping review. Afr J Prim Health Care Fam Med 2022;14(1):e1–11. [CrossRef]
[Pubmed]
26.
Kang HK. Influence of culture and community perceptions on birth and perinatal care of immigrant women: Doulas’ perspective. J Perinat Educ 2014;23(1):25–32. [CrossRef]
[Pubmed]
27.
Stephenson J, Heslehurst N, Hall J, et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018;391(10132):1830–41. [CrossRef]
[Pubmed]
28.
Chuang CH, Velott DL, Weisman CS. Exploring knowledge and attitudes related to pregnancy and preconception health in women with chronic medical conditions. Matern Child Health J 2010;14(5):713–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Lucky Oseghale Oloboh - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shiphrah Kuria-Ndiritu - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Esther Nduku Muia-Matuku - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Lucky Oseghale Oloboh et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}